Multicenter
Cooperative Collaborative Action Research Study
in the Philippines
(MCCCARS)
2002
Reynaldo O. Joson, MD, MHA,
MHPEd, MS Surg
Program Director
Email: rjoson@maniladoctors.com.ph
|
Identified Problem | |
|
Is a recumbent plain abdominal x-ray (without an upright film) sufficient in the evaluation of patients with acute intestinal obstruction? |
October, 2002
|
Started |
Target Date of Completion |
|
May, 2002 |
August, 2002; October, 2002 |
|
For late comers, who want to catch
up, | |
|
|
|
|
|
Steps in Action Research |
Activities/Results |
Time Table |
|
1. Analysis of the problem |
| |
|
2. Research designs on how to solve the problem |
| |
|
3. Implementation of action plan |
Implementation of Research Methods |
Deadline:October 1, 2002 |
|
4. Evaluation of results of implementation |
|
October 5, 2002 |
Draft of Proposal/Paper
Title:
Is a recumbent plain abdominal x-ray (without an upright film) sufficient in the evaluation of patients with acute intestinal obstruction?
A Preliminary Report
Authors:
Members of MCCCARS who ACTIVELY participated in the study will be cited as authors.
Members of MCCCARS who contributed opinions in the study will be acknowledged.
The centers will be acknowledged.
Multicenter Cooperative Collaborative Action Research Study (MCCCARS) Group
Centers:
Ospital ng Maynila Medical Center (OMMC), Manila Doctors Hospital (MDH), Zamboanga City Medical Center (ZCMC); Batangas Regional Hospital (BRH); Davao Regional Hospital (DRH), Philippine General Hospital (PGH); Region I Medical Center; Palawan Provincial Hospital (PPH); Visayas Community Medical Center (VCMC)
MCCCARS Members
Reynaldo Joson, MD; Edgardo Penserga, MD; Harry Go, MD; Adrian Yu, MD; Ravel Bartolome, MD; Alfonso Nunez, MD; Alex Cerrillo, MD; Alex Palines, MD; Alex Tan, MD; Manuel Francisco Roxas, MD; Noneng Monroy, MD; Roberto Valenzuela, MD; Dionisio Cruz, MD; Roehl Salvador, MD; Ricky Torres, MD; Rogelio G. Kangleon, Jr, MD
OMMC Residents: Ana Llado, MD; Alfred Troncales, MD; Marlou O. Padua, MD; Romero D. Dangoy, MD
MDH Resident: Ric Naval, MD
Abstract:
A multicenter cooperative and collaborative action research study (MCCCARS) was conducted to determine if a recumbent plain abdominal x-ray is sufficient in diagnosing patients with acute intestinal obstruction. The specific objectives consisted of the following: 1) to compare the likelihood ratios of air-fluid levels on upright films and generalized bowel distention with absence of gas in the rectosigmoid on recumbent films; 2) to get a survey among radiologists on use and interpretation of plain abdominal x-rays; 3) to formulate a clinical algorithm using recumbent plain abdominal x-ray only; and 4) to validate the algorithm as to accuracy. Tools for data gathering included literature search, focused group discussion, surveys and questionnaires, retrospective chart reviews, and prospective data accrual. Results show that the likelihood ratio of air-fluid level was only 2 whereas that of generalized bowel distention without gas in the rectosigmoid area was about 70. The radiologists considered generalized bowel distention without gas in the rectosigmoid as the most reliable sign of mechanical intestinal obstruction. The initial validation study of the clinical algorithm without the use of an upright film showed 100% accuracy. This is a preliminary report. However, the evidences on hand seem to be strong enough to indicate that a recumbent plain abdominal x-ray will be sufficient.
Keywords: intestinal obstruction, abdominal x-ray, air-fluid levels
Introduction:
In the evaluation of patients with acute intestinal obstruction, after the interview and physical examination, the usual paraclinical diagnostic procedure being requested by clinicians globally(1) including the Philippines (per email communication with members of multicenter study group and per survey of radiologists - see appendix) is an abdominal x-ray in 2 different positions, namely: recumbent and upright or lateral decubitus position.
In the recumbent x-ray, distention of bowels, its degree, pattern and distribution, is sought for in aid of the diagnosis of acute intestinal obstruction and its cause, either mechanical or non-mechanical or adynamic ileus. In the upright or decubitus x-ray, an air-fluid level is sought for.
In the institutions of most of the authors (except for ZCMC), 2 films corresponding to a recumbent and upright or lateral decubitus positions have been routinely used in the radiologic examination of the abdomen in patients with suspected acute intestinal obstruction. Recently, the authors poised the question whether a recumbent plain abdominal x-ray would be sufficient. The question aroused from the realization that air-fluid level is not pathognomonic for mechanical obstruction; that diagnosis of intestinal obstruction relies primarily on clinical symptoms and signs, and secondarily on abdominal x-ray; and that a recumbent plain film supplies more diagnostic information than an upright or lateral decubitus film and may be sufficient as a paraclinical diagnostic procedure. The experience that air-fluid level is not pathognomonic for mechanical obstruction is supported by some papers in the literature (2-4).
As a result of this question, an action research study was conducted with the general objective of determining whether a recumbent plain abdominal x-ray would be sufficient without having to request for an upright or lateral decubitus film in the evaluation of patients with acute intestinal obstruction.
Objectives:
The specific objectives consisted of the following:
1. To determine the sensitivity, specificity, and likelihood ratios of radiologic air-fluid level on upright or lateral decubitus position in patients with acute intestinal obstruction.
2. To determine the sensitivity, specificity, and likelihood ratios of generalized bowel distention with absence of gas in the rectosigmoid area on recumbent plain x-ray of the abdomen in patients with acute intestinal obstruction.
3. To get a survey among radiologists on the use and interpretation of plain films of the abdomen in patients with possible intestinal obstruction.
4. To formulate an algorithm that utilizes data obtainable from history, physical examination, and recumbent plain abdominal x-ray only in evaluating patients with acute intestinal obstruction.
5. To validate the algorithm as to accuracy.
General Methodology:
The concept and methodology of an action research (5-6) was utilized, namely: analysis of the problems, research designs on how to solve the problems; implementation of action plan; and evaluation of results of implementation. Multicenter cooperation and collaboration was tapped for data gathering, patient accrual, and validity testing of proposed solution. (Multicenter cooperation and collaboration does not necessary mean that all centers were accomplishing the same thing at the same time and all the time. Cooperation and collaboration was utilized when some centers could not, because of logistic and technical problems, accomplish certain research objectives while some centers could.) Tools for data gathering included literature search using evidence-based approach, focused group discussion among the members of the multicenter cooperative collaborative action research study (MCCCARS) group, surveys and questionnaires, retrospective chart reviews, and prospective data accrual. Focused group discussion done mainly through email was the tool used for consensus gathering for problem-solving and decision-making. Appropriate statistics, both descriptive and analytical, were used as needed.
Specific Methods for Each Objective:
Objectives 1 and 2:
Literature search using an evidence-based approach, focused group discussion among the members of the MCCCARS group, surveys and questionnaires, retrospective chart reviews, and prospective data accrual were used to gather data for objectives 1 and 2.
A retrospective chart review conducted in hospital A included 81 adult patients operated on for acute intestinal obstruction from January, 1996 to December, 2000. The age ranged from 18 to 75 years old with a mean age of 44 years old. The sex distribution was 58 males and 23 females. The sensitivity, specificity, and likelihood ratios of air-fluid levels and generalized distention of bowels associated with absence of gas in the rectosigmoid were computed using the operative findings as gold standards.
A prospective study conducted in hospital B included 29 adult patients evaluated for acute intestinal obstruction from January, 2002 to June, 2002. The age ranged from 16-89 years old with a mean age of 51 years old. The sex distribution was 14 males and 15 females. The sensitivity, specificity, and likelihood ratios of air-fluid level and generalized distention of bowels associated with absence of gas in the rectosigmoid were computed using operative findings and observation as gold standards for operated and non-operated patients respectively.
Objective 3:
Radiologists from 5 different centers were requested to answer a questionnaire that was formulated to bring out their use and interpretation of the plain films of the abdomen in patients with possible acute intestinal obstruction. A total of 19 radiologists from 5 institutions submitted answers to the questionnaire.
Objective 4:
Focused group discussion and consensus gathering was done and based on the results of objectives 1 to3, an algorithm was formulated.
Objective 5:
Prospective data gathering was done to validate the algorithm formulated in objective 4. From January, 2002 to July, 2002 at hospital A, the algorithm without an upright film was used in the evaluation of patients with possible obstruction. Fourteen patients were accrued with age ranging from 14 to 56 years old and a sex distribution of 10 males and 4 females. The diagnostic accuracy rate was determined using the operative findings and observation as gold standards for operated and non-operated patients respectively.
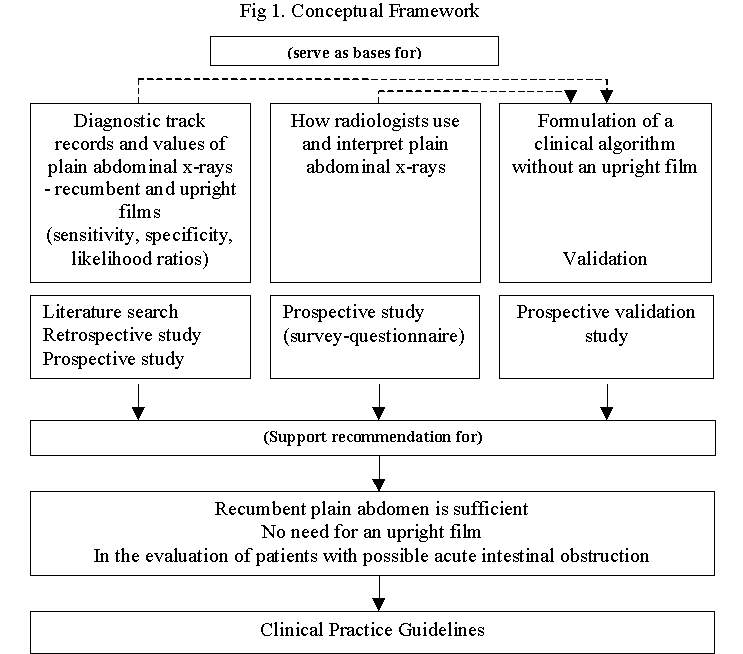
The conceptual framework of this action research is illustrated in Figure 1.
Results
Objective 1:
The sensitivity and specificity rates of air-fluid levels ranged from 52 to 73% and 40 to 71% respectively (Table 1). The likelihood positive ratios ranged from 1.21 to 2.1.
Table 1: Sensitivity, specificity, and likelihood ratios of radiologic air-fluid level.
|
|
Sensitivity |
Specificity |
Likelihood+ Ratio |
Likelihood- Ratio |
|
Harlows(2) |
52% |
71% |
1.79 |
0.67 |
|
MCCCARS (hospital A) |
73% |
40% |
1.21 |
0.67 |
|
MCCCARS (hospital B) |
63% |
70% |
2.1 |
0.52 |
Objective 2:
No paper in the literature was found that could give the sensitivity, specificity, and likelihood ratios of radiologic signs of intestinal obstruction on recumbent plain abdominal x-ray. The rates were computed from the local studies.
The sensitivity and specificity of generalized bowel distention with absence of gas in the rectosigmoid area were 70% and 100% respectively (Table 2A). The positive predictive value was 100% and the positive likelihood ratio was ~70.
In the absence of generalized bowel distention on recumbent film, nongeneralized or segmental bowel distention may be seen in patients with acute intestinal obstruction, either with or without gas in the rectosigmoid area. A computation of the sensitivity and specificity of nongeneralized bowel distention with absence of gas in the rectosigmod area was 33% and 62% (Table 2B). The positive likelihood ratio was 0.49.
Table 2A: Sensitivity, specificity and likelihood ratios of generalized bowel distention with NO gas in the rectosigmoid area in patients with acute intestinal obstruction (hospital B data).
|
|
Mechanical Obstruction |
Non-Mechanical Obstruction |
|
|
Diffuse distention with NO gas |
7 |
0 |
7 |
|
Diffuse distention with gas |
3 |
1 |
4 |
|
|
10 |
1 |
11 |
Sensitivity = 70%
Specificity = 100%
Positive predictive value = 100%
Negative predictive value = 25%
Likelihood ratio = ~70
Table 2B: Sensitivity, specificity, and likelihood ratios of segmental distention with no gas in the rectosigmoid area in patients with acute intestinal obstruction (hospital B data).
|
|
Mechanical Obstruction |
Non-Mechanical Obstruction |
|
|
Segmental distention with NO gas |
3 |
3 |
6 |
|
Segmental distention with gas |
6 |
5 |
11 |
|
|
9 |
8 |
17 |
Sensitivity = 33%
Specificity = 62%
Positive predictive value = 50%
Negative predictive value = 45%
Likelihood ratio = 0.49
Objective 3:
A total of 19 respondents from 5 different institutions answered the questionnaire we formulated regarding their use and interpretation of plain films of the abdomen in patients with possible intestinal obstruction. Hospital A had 4 respondents, hospital B with 5, hospital C with 4, hospital D with 2 and hospital E with 4. Based on their answers (Table 3), most of them agreed that a lot of physicians would still request 2 views of the abdomen whenever they are entertaining a case of an acute intestinal obstruction. Though most of the respondents said that air fluid level is not pathognomonic of mechanical obstruction and that they see bowel distention more often than air fluid level in a mechanical obstruction, majority of them still believed that 2 views are still necessary in diagnosing mechanical obstruction. For most of the radiologists, diffuse bowel distention with no presacral or rectosigmoid gas is the most reliable sign of mechanical obstruction, while diffuse bowel distention with presacral or rectosigmoid gas is the most reliable sign for non-mechanical obstruction.
Respondents:
OMMC = 4
MDH = 5
Zamboanga City = 4
Batangas Regional Hospital = 2
Philippine General Hospital = 4
Davao = 4
Table 3. Results of survey of radiologists on use of upright and recumbent films of abdomen in patients with possible acute intestinal obstruction.
|
|
YES |
NO | ||||||
|
The usual x-rays being requested by clinicians for patients with possible acute intestinal obstruction are recumbent and upright (or lateral decubitus) plain x-ray of the abdomen. |
21 |
2 | ||||||
|
If there are already air-fluid levels on upright or lateral decubitus film, there are usually distended small bowels on the recumbent film. |
18 |
5 | ||||||
|
If there are distended small bowels on the recumbent film, there may or may not be air-fluid levels on the upright or lateral decubitus film. |
21 |
2 | ||||||
|
Is the presence of a differential air-fluid level on upright or lateral decubitus film by itself pathognomonic or has a 100% specificity for mechanical intestinal obstruction? |
2 |
20 | ||||||
|
From your point of view as a radiologist, do you think that a recumbent plain abdomen correlated with clinical signs and symptoms is sufficient (without an upright film) for the clinician to make a diagnosis of acute intestinal obstruction with an accuracy of more than 95%? |
10 |
13 | ||||||
|
|
< 25% |
>25<50% |
>50<90% |
>90% | |||||
|
In your experience, how often do you see differential air-fluids in the radiology of patients with possible acute intestinal obstruction? |
1 |
4 |
16 |
2 | |||||
|
In your experience, how often do you see distended bowels in the radiology of patients with possible acute intestinal obstruction? |
1 |
0 |
8 |
14 | |||||
|
Most reliable sign for |
Mechanical Obstruction |
Non-Mechanical Obstruction | |
|
diffuse distention of small bowels with gas in the rectosigmoid or presacral area |
1 |
17 | |
|
diffuse distention of small bowels with NO gas in the rectosigmoid or presacral area |
11 |
0 | |
|
segmental distention of small bowels with gas in the rectosigmoid or presacral area |
0 |
5 | |
|
segmental distention of small bowels with NO gas in the rectosigmoid or presacral area |
3 |
0 | |
|
differential air-fluid level |
7 |
0 | |
|
|
Primary Radiologic Diagnosis | ||||||
|
Case |
Radiologic findings on Plain Abdomen, recumbent and upright |
Mechanical Obstruction |
Adynamic Ileus |
No Obstruction | |||
|
1 |
(-) distended small bowels |
0 |
1 |
22 | |||
|
2 |
(-) distended small bowels |
0 |
5 |
13 | |||
|
3 |
(+) distended small bowels |
0 |
21 |
0 | |||
|
4 |
(+) distended small bowels |
0 |
22 |
1 | |||
|
5 |
(+) distended small bowels |
11 |
11 |
0 | |||
|
6 |
(+) distended small bowels |
9 |
12 |
1 | |||
|
7 |
(+) distended small bowels |
10 |
11 |
1 | |||
|
8 |
(+) distended small bowels |
22 |
1 |
0 | |||
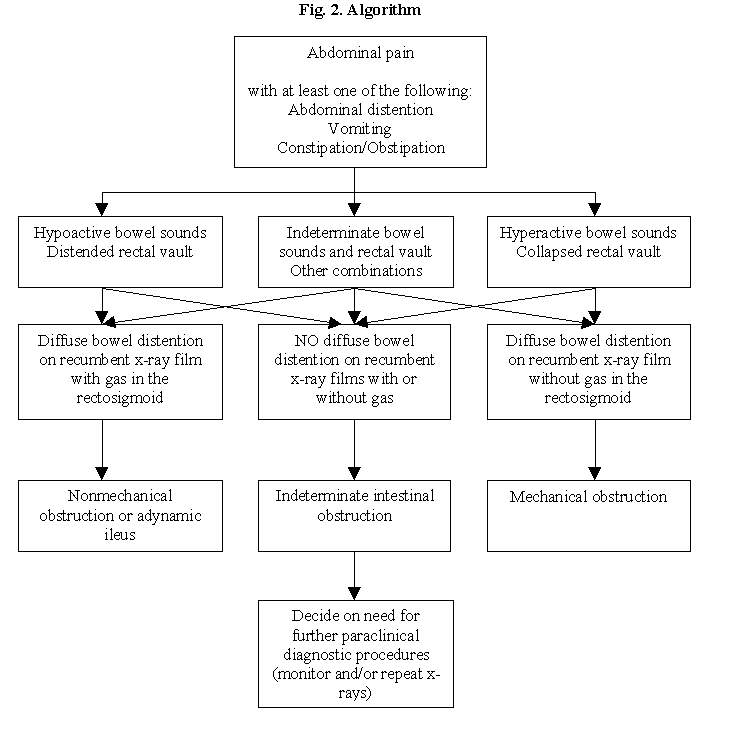
Objective 4:
After considering all the evidences gathered in objectives 1 to 3 in a focused group discussion and consensus gathering, with some support from the literature (7), a clinical algorithm was formulated utilizing data obtainable from history, physical examination, and recumbent plain abdominal x-ray in evaluating patients with acute intestinal obstruction. See Fig 2.
Objective 5:
The clinical algorithm was validated in terms of accuracy and utility. A total of 14 patients have been accrued and so far, there was 100% accuracy in the diagnosis of mechanical obstruction and non-mechanical obstruction (see Table 4).
Table 4: Algorithm accuracy and validity
|
|
Mechanical Obstruction |
Non-Mechanical or NO Obstruction |
|
|
Mechanical Obstruction |
8 |
0 |
8 |
|
Non-Mechanical or NO Obstruction |
0 |
6 |
6 |
|
|
8 |
6 |
14 |
Discussion:
This is a preliminary report awaiting more data to come in, particularly in the multicenter validation of a proposed clinical algorithm relying on clinical data and just a recumbent plain abdominal x-ray in the evaluation of patients with possible acute intestinal obstruction. Short of more validation data, however, the evidences brought forth by this action research seem to be strong enough to indicate that a recumbent plain abdominal x-ray will be sufficient.
Looking at the conceptual framework of the research (Fig.1), the diagnostic track records and values of recumbent and upright abdominal films, the result of the survey from the radiologists, and the initial validation results on the clinical algorithm are all supporting the recommendation for non-inclusion of an upright film anymore.
In the diagnostic track records and values of the two x-ray films, the likelihood ratio of air-fluid level in an upright film is low at 2 for mechanical intestinal obstruction whereas the likelihood ratio of a generalized bowel distention with absence of gas in the rectosigmoid area on a recumbent film is high at almost 70. This difference in likelihood ratio is enough to favor a recumbent film over an upright film. Furthermore, the low likelihood ratio of an air-fluid level is enough to recommend that it is no longer necessary to request for an upright film after a recumbent film is done because it will not significantly affect the pretest-probability.
These arguments can be illustrated by some clinical examples.
If after history and physical examination, the pre-test probability is about 60%, 70% or even 80%, and there is a need for a paraclinical diagnostic procedure, either a recumbent or an upright plain abdominal x-ray, what should be recommended? The recumbent plain abdomen is usually the initial x-ray to request because right away, the x-ray can tell whether bowel distention is present or not, and if present, the degree of distention, whether generalized or non-generalized (or segmental). Gas in the rectosigmoid area can also be studied. If a generalized bowel distention with absence of gas in the rectosigmoid is seen, with the likelihood ratio of 70, the recumbent plain abdomen will be able to increase the pre-test probability to a post-test probability as high as 98-99% that there is no need for an upright film anymore. With a likelihood ratio of 2, the air-fluid level on an upright film will no longer significantly increase the high post-test probability after a recumbent film is done.
Suppose the recumbent plain abdomen does not reveal generalized bowel distention, should an upright film be requested? The answer is still no since chances of seeing an air-fluid level in an upright film in nondistended bowels are small. Furthermore, the likelihood ratio of 2 of air-fluid level, if present, will not significantly affect the pre-test probability.
In the survey of radiologists, the tendency to still look for an air-fluid level in an upright film despite the belief that the degree of distention of the bowel and presence or absence of gas in the rectosigmoid in the recumbent film is the most reliable cue to differentiate between mechanical and non-mechanical obstruction is more of a habit.
The initial validation data from hospital A showing a 100% diagnostic accuracy rate of a clinical algorithm without the use of an upright film tend to support the contention that a recumbent film is sufficient. With all the limitations of gathering data (with questions of validity and reliability, especially of secondary data) on the sensitivity and specificity of the radiologic signs of obstruction both on recumbent and upright films of the abdomen, the consensus of the MCCCARS members is that the final evidence that will be needed to really say that a supine film is sufficient is the validation data from various centers that will omit the use of the upright films in the evaluation of patients with possible acute intestinal obstruction. Hospital C has not been using upright films since 1993. Short of documenting the diagnostic accuracy rate of this practice, the chairperson claims an accuracy rate as high as 95%.
If indeed an upright film is not needed anymore, the benefit of this study is cost-reduction not only on the part of the government hospitals that have meager resources but also on the part of the paying patients.
Once the algorithm is validated, the plan is to institutionalize it by incorporating it into the clinical practice guidelines of the department and the hospital. A memo of understanding with the Department of Radiology will be formulated and signed. A memo to the Department of Surgery staff will be issued with the following content:
· NO NEED TO REQUEST FOR AN UPRIGHT FILM OF THE ABDOMEN IN PATIENTS WITH POSSIBLE ACUTE INTESTINAL OBSTRUCTION.
· IF A PARACLINICAL DIAGNOSTIC PROCEDURE IN THE FORM OF AN X-RAY OF THE ABDOMEN IS NEEDED, A SUPINE FILM IS SUFFICIENT.
On the Multicenter Cooperative Collaborative Action Research Methodology
The action research methodology used in this project followed the concept as defined by Cohen and Manion (6.7), that is, "small scale intervention in the functioning of the real world and a close examination of the effects of such intervention." It is situational in that it is concerned with diagnosing a problem in a specific context and attempting to solve it in that context. Usually collaborative teams of researchers and practitioners work together on a project. It is participatory in the sense that the team members themselves take part directly or indirectly by implementing the research. Lastly, it is self-evaluative in that modifications are continually evaluated within the ongoing situation, the ultimate objective being to improve practice in some way or another.
While experimental research is concerned mainly with establishing relationships and testing theories, action research has as a focus a specific problem in a specific setting. It makes no attempt to identify one particular factor and study it in isolation divorced from the context giving it meaning.
As Margules (7) points out, "in combining action processes (planning, implementation, and evaluation) with research processes (problem identification, hypothesis formation, and testing), the result is a sequence of steps and activities that identify the relevant events that must happen in the initiation and implementation of change."
The essential steps in action research are the following:
1. Analysis of the problems
2. Research designs on how to solve the problems
3. Implementation of action plan
4. Evaluation of results of implementation
In the Philippines, most of the medical researches done are NOT of the action research type. Thus, their utility just end in being published in journals. They are NOT being used by the people in the institution of origin of the research papers. More so, they are NOT being used by people outside the institution of origin.
The other problems in conducting research projects in the country are the number of clinical subjects and lack of resources.
This action research has shown how a real world problem was being solved systematically, cooperatively, and collaboratively. The multicenter cooperative and collaborative effort has illustrated the advantages of sharing of resources. The ultimate impact of this action research consists of solutions of problems and implementation of improvement measures in patient care being simultaneously undertaken in several centers in the country.
Unfinished tasks:
1. Multicenter validation of a clinical practice guideline without the use of an upright film
2. Continuous search and incorporation of new data to refine and strengthen the information on hand
3. Institutionalization of the validated clinical practice guidelines in various centers
References:
5. Cohen L, Manion L: Research Methods in Education. London, Croom Helm, 1980.
6. Marguiles N: Managing change in health care organization. Medical Care 1977;15:693-704.
7. Bohner H, Yang Q, Franke C, Verreet PR, Ohmann C. Simple data from history and physical examination help to exclude bowel obstruction and to avoid radiographic studies in patients with acute abdominal pain. Eur J Surg 1998 Oct;164(10):777-84.
Questions for members to answer:
A recumbent and an upright plain abdominal x-ray are usually requested by clinicians in the evaluation of patients with possible acute intestinal obstruction. What is your present practice when you need an x-ray of the abdomen in such patients?
o Recumbent and upright
o Recumbent only
o Upright only
Results so far (as of June 16, 2002):
Surgeons:
4 surgeons - routine recumbent and upright (1 still has the habit but in decision-making, relies more on supine and clinical data)
2 surgeons - recumbent only
Institutional practice:
All routine recumbent and upright except for Zamboanga City Medical Center as of 1991 and Ospital ng Maynila Medical Center as of 2001.
The following are still practicing routine recumbent and upright requesting:
Philippine General Hospital
Jose Reyes Memorial Hospital
Manila Doctors Hospital
Region I Medical Center
Davao Regional Hospital